There has been plenty of research over the past several years examining the concept of movement variability(1,2,3) in regards to healthy human movement. At the same time, an abundance of research has also been undertaken looking into the optimal(4,5,6) movement patterns that are necessary for safe movement practices.
To clarify let’s put some general definitions around these two concepts:
Movement variability can be described as differences in observed motions when performed in the same situation(2), or (and I like this one adapted from Webster’s(7)) “the power possessed by living organisms, both animal and vegetable, of adapting their physical movements to modifications or changes in their environment”.
Movement optimization can be defined as the best practice of performing specific human motions in regards to physical health and longevity. At first glance these two concepts seem contradictory to each other, but I don’t quite see it that way. As I see it, these two concepts need to be linked in order for us to get the most out of our movement practices.
I would like to set forth some general guidelines in order to better understand how these two important perspectives can be utilized in conjunction with one another to allow for healthy movement.
1) Understand which positions/movements have been shown to lead to injury in scientific literature (8-12):
These positions include but are not limited too: pes planus (flat feet), genu valgum (knock knees), anterior pelvic tilt (overextended lower back), kyphosis of the thoracic spine (humpback), anterior translation of he humerus on the glenoid fossa (forward shoulders), and protrusion of the cervical spine (forward head position). Research has shown these positions to be associated with higher risks for overuse injuries to the spine, shoulders, knees and feet.

Excessive forward head and shoulder position, along with an excessive anterior pelvic tilt have been associated with increased risk for spine and shoulder pain
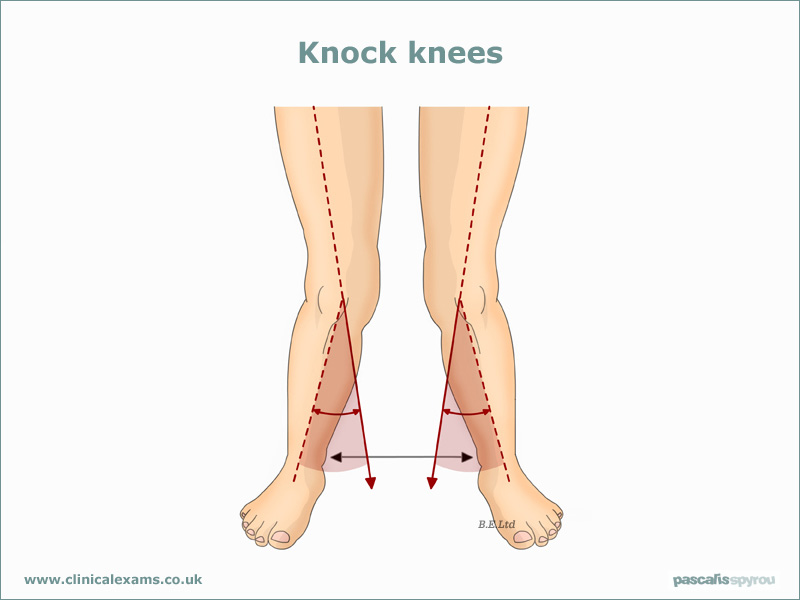
Genu valgum (knock knees) and pes planus (flat feet) are associated with increased risks for lower extremity overuse injuries
2) Understand that the above positions/movement patterns are often caused by lack of movement variability:
This is to say that these positions/movement patterns are not inherently “bad or evil”, it is just that they are frequently positions one takes due to movement invariability. For example, forward head and shoulder posture, along with thoracic kyphosis are often the result of sitting for extended periods of time. Moreover, sitting for extended periods also tends to shorten the hip musculature multi-directionally leading to anterior pelvic tilt, genu valgum (hip internal rotation/adduction motion), and pes planus (secondary to genu valgum). Standing for long durations is no better, as it tends to lead to anterior rotation of the pelvis and lumbar hyperextension. Moreover, standing and walking with overly supportive shoes casts the foot in the same position all day, which often leads to pes planus. Often this invariability of movement starts at a very young age (i.e. as soon as children are put in supportive shoes and chairs). Therefore, chronic non-movement can be seen as one of the root causes of poor positioning/movement.

Slumped chair sitting often leads to tight hip flexors which leads to an anterior rotation of the pelvis when standing. Moreover, this position promotes forward head and shoulder posture as well as a kyphotic (rounded) upper back.

Sneakers with excessive support can often lead to pes planus by limiting foot/ankle mobility as well as creating disuse atrophy (weakness) in the muscles that support the medial arch of the foot. Treatment for this is often to add more support to the arch further perpetuating a vicious cycle of tight, weak and uncoordinated feet and ankles.
3) Understand which situations are most appropriate for specific optimal movement patterns, and in which situations more movement variability is warranted:
This speaks to the importance of understanding which movement patterns and positions are most stable for the physiological structure of the human body. The above mentioned postures that are found to lead to injury, are all unstable/unbalanced positions. That is to say that they put less resilient structures (joints, cartilage, ligaments) on more stress than the more resilient and adaptive musculature. With this understanding, it is important to note that certain movement situations do not necessarily call for the most stable position of the musculature. In fact, often energy conservation is a more effective strategy with activities of daily living.

With low load tasks, energy conservation, even in the absence of ideal positioning, may be the best strategy for decreasing physical stress to the body.
This means that doing what feels easiest may actually decrease stress to physical structures, as opposed to taking the effort find a “perfect position”. The key is to identify and differentiate situations where optimal stability is more warranted, versus when energy conservation is the better strategy. Obviously, lifting heavy stuff should fall into the “better be stable” category. This category includes weight training, but also includes challenging body weight movements, moving furniture/luggage and movements that are done at high volumes.
Examples of situations where optimal positioning can be temporarily abandoned are when cautiously exploring full ranges of motion at various joints during movement practices such as yoga, martial arts, gymnastics, and dance, or during transitions such as getting up off the floor or rolling in bed/on the ground.

Back bending is an example of an imbalanced position that can be cautiously explored by certain populations in order to improve spinal mobility necessary for higher level activities. Due to the excessive shortening of the back of the body and subsequent lengthening of the front of the body, it is very difficult to find muscular stability in this position and will be more likely to cause injury if performed at high volumes.

A child sitting in a squat with a slight knock kneed and flat footed position is a common example of conserving energy by resting on the joints and ligaments. This strategy gets riskier with age as these structures get less resilient.
References:
1.Harbourne, R., & Stergiou, N. (2009). Movement Variability and the Use of Nonlinear Tools: Principles to Guide Physical Therapist Practice. Physical Therapy, 89(3), 267-282.
2.http://users.speakeasy.net/~wrayre/pubs/VariabilityinHumanBehaviorModelingWrayLairdBRIMS2003.pdf
3.Stergiou, N., Harbourne, R., & Cavanaugh, J. (2006). Optimal movement variability: A new theoretical perspective for neurologic physical therapy. J Neurol Phys Ther., 30(3), 120-129.
4.Glazier, P., & Davids, K. (2009). Constraints on the Complete Optimization of Human Motion. Sports Medicine, 39(1), 15-28.
5.Kaphle, M., & Eriksson, A. (2008). Optimality in forward dynamics simulations. Journal of Biomechanics, 41(6), 1213-1221.
6.http://www.functionalmovement.com/articles/research/2011-03-07researchstatementandreview (literature review on the FMS: screen for looking at more optimal movement patterns)
7.http://www.webster-dictionary.net/definition/variability
8.Kaufman, K., Brodine, S., Shaffer, R., Cullison, T., & Johnson, C. (1999). The Effect of Foot Structure and Range of Motion on Musculoskeletal Overuse Injuries. Am J Sports Med, 27(5), 585-593.
9.Cowan, D., Jones, B., Frykman, P., Polly, D., Harman, E., Rosenstein, R., & Rosenstein, M. (n.d.). Lower limb morphology and risk of overuse injury among male infantry trainees. Medicine & Science in Sports & Exercise, 945-952.
10.Krivickas, L. (n.d.). Anatomical Factors Associated with Overuse Sports Injuries. Sports Medicine, 132-146.
11.Griegel-Morris, P., Larson, K., Oatis, C., & Mueller-Klaus, K. (1992). Incidence of Common Postural Abnormalities in the Cervical, Shoulder, and Thoracic Regions and Their Association with Pain in Two Age Groups of Healthy Subjects. Physical Therapy, 72(6), 425-431.
12.Christie, H., Kumar, S., & Warren, S. (n.d.). Postural aberrations in low back pain. Archives of Physical Medicine and Rehabilitation, 218-224.